
https://www.lewrockwell.com/2015/04/bretigne-shaffer/first-they-came-for-the-anti-vaxxers/
Earlier this year I spent a few days at the Ronald Reagan UCLA Medical Center with my daughter who was having an EEG done. On our way home, I learned that there had been an outbreak of an antibiotic-resistant bacteria while we were there, that it had infected seven people and killed two of them. My daughter and I were fine – the infection having been limited to people using a particular kind of duodenoscope.
When the story hit the news, I fully expected nationwide outcry similar to that inspired by the recent measles “epidemic” that began at Disneyland. That outbreak killed no-one, yet set the country on fire with calls for mandatory vaccination and even prison sentences for parents who choose not to vaccinate their children. Drug-resistant “superbugs” kill nearly 15,000 people a year in the US and a recent report predicts that they could kill as many as 300 million people by 2050. Surely this far more deadly health threat would lead to similar widespread outrage and calls for those even remotely responsible to be held accountable.
I expected to see editorials calling for anyone who engaged in the overuse of antibiotics to be shunned by society; doctors who prescribed them unnecessarily (around 50% of all prescriptions by some estimates) to be censured and perhaps lose their licenses; parents who asked for antibiotics every time their child had an ear infection – despite the fact that the vast majority are not bacterial and are unaffected by antibiotics – to be thrown in jail for endangering the rest of us. But I saw nothing along these lines. Why not?
The manipulation of the conversation around vaccines in the mainstream media has been nothing short of a tour de force. If you read only mainstream publications, you might come away with the impression that outbreaks of measles are the most serious public health crisis since the Black Death. You might think that those who do not vaccinate are uneducated, superstitious, “anti-science” zealots who get their information from daytime talk shows. You might even start to feel outrage at these people who – for no good reason at all – have decided to endanger everyone else by refusing to do what every doctor knows is perfectly safe, effective and the socially responsible thing to do.
The presentation of this issue has been a study in just how easy it can be to generate mass hysteria around a particular threat – even while much more serious threats inspire no such response. It’s as if every mainstream reporter has been given the same playbook to use in putting together their articles about vaccines – a playbook designed to elicit the above response from the public. I’ve tried to imagine what this playbook must look like and I think I’ve come up with a pretty decent facsimile. Here it is, along with my own annotations:
1. Make it clear that parents who choose not to vaccinate their children are only getting their information from Jenny McCarthy, Jim Carey and other celebrities with absolutely no scientific credentials.
Pretend that doctors and scientists who are critical of vaccines – doctors like Dr. Suzanne Humphries, Dr. Robert Sears, Dr. Kenneth Stoller, Dr. Robert Rowen, Dr. Janet Levatin, Dr. Stephanie Cave, Dr. Sherri Tenpenny, Dr. Meryl Nass, Dr. Jay Gordon, Dr. Jane Orient, and many of the members of the Association of American Physicians and Surgeons, CDC researcher Dr. William Thompson, and all of the doctors and scientists listed here and here – don’t exist. Because really, if you don’t write about them, they don’t.
2. Always equate the views of the CDC, medical journals and pharmaceutical company spokespeople with “science.” Some people will try to tell you that science is a method, not a conclusion, that scientific truths cannot be determined by consensus or by appeal to authority, but you can just ignore them.
As one (self-proclaimed) scientist put it:
“In my personal and scientifically backed opinion, the war against disease is a hundred fold more important than the mum-led war against vaccines. Do you want your child to die a slow, painful, agonizing death? If not, then shut the f*** up with your so called ‘facts’ you got from Yahoo Answers and get your kid vaccinated.
“I am going to sound derogatory, but if you don’t have formal education in at least biology, you have no role to talk about the way vaccines should be done.” (Sic.)In other words, if you don’t have the same training we do, you don’t get to be part of the discussion. Even when the topic of that discussion is whether or not we get to forcibly inject things into your bodies and the bodies of your children. Just shut up and trust the scientists. But not these scientists – they are all anti-science scientists. Only trust these ones.
3. Remind your readers that, however heart wrenching or tragic, anecdotal accounts are just that. They are not scientific, they don’t say anything about relative risk, and should play no role in influencing your opinion about vaccines.
Until you want to tell them the heart wrenching story of how author Roald Dahl lost his daughter to measles, or about the death of a young girl from rotavirus that inspired Dr. Paul Offit to develop a vaccine for that disease.
Anecdotal accounts of people suffering from vaccine-preventable illnesses are fine. Anything else though is just irrational. Take for example the thousands of stories from parents whose children were perfectly healthy until they received one or more vaccines and then suddenly lost the ability to speak, to walk, to feed themselves, or who started having seizures, stopped breathing or died. Many of the parents in these cases report that their doctors insist the vaccines had nothing to do with their child’s injury, even when no other explanation is apparent. Indeed, the vaccine manufacturers and the CDC insist that most such cases are simply coincidences and have nothing to do with the vaccines. But given the well-documented degree of conflict of interest and fraudulent practices within the CDC and the medical research community as a whole, many parents are understandably skeptical of such claims.
4. Remind your readers that “correlation is not causation.”
Unless you want to show them this graph and tell them it proves that vaccines save lives:
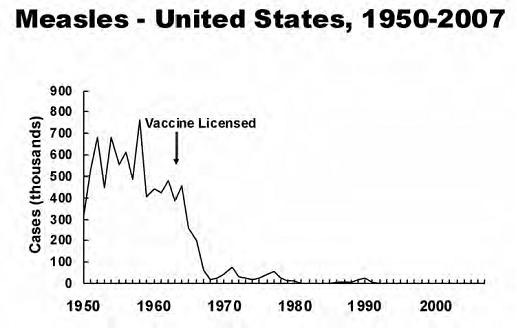
Whatever you do though, make sure you don’t accidentally show them this graph instead:
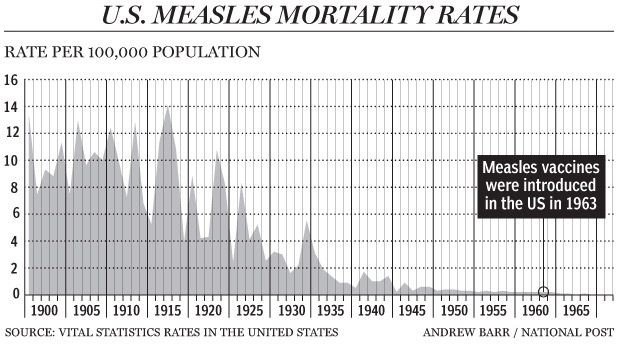
By the 1950s in the United States though, measles was considered a mild childhood disease that nearly everyone caught before adulthood and lived through with no serious consequences. Says Dr. Donald Miller:
“With good sanitation and nutrition, the pre-vaccine mortality rate of measles in the U.S. was less than 1 in a million (compared with 14 deaths per 100,000 in 1900); seizures occurred in 1 in 3,000 people; and encephalitis, 1 in 100,000, with full recovery in 75 percent of those cases.”It is also worth noting that the CDC’s statement that “(f)or every 1,000 children who get measles, one or two will die from it” relies on reported cases of measles. A more accurate estimate puts the death rate at closer to 1 out of 10,000 cases.
Meanwhile, in the past ten years there have been only a handful of measles deaths in the US, but VAERS data report 109 deaths associated with the measles vaccine since January of 2004, and the US Court of Federal Claims has settled 111 claims related to harm from the MMR vaccine in that same time.
Not only is measles a relatively benign illness for healthy people living in developed countries, contracting and surviving the disease confers benefits to the immune system – as well as strengthening herd immunity – in ways that vaccines cannot.
Far from protecting the most vulnerable demographic groups, widespread vaccination has increased the risk of serious harm from measles in some of these populations: Infants and very young children, as well as adults. Normally, measles wouldn’t appear in these age groups – but now it does, thanks to the vaccine. As Lawrence Solomon reported in the Financial Post last year:
“In the pre-vaccine era, when the natural measles virus infected the entire population, measles — ‘typically a benign childhood illness,’ as Clinical Pediatrics described it — was welcomed for providing lifetime immunity, thus avoiding dangerous adult infections. In today’s vaccine era, adults have accounted for one quarter to one half of measles cases; most of them involve pneumonia, one-quarter of them hospitalization.As discussed below, childhood illnesses like measles and mumps can help to develop the immune system in ways that help to protect against things like asthma, autoimmune disease and even cancer. So the proposition that eliminating measles – rather than simply reducing its deadliness – is a worthy public health goal is a questionable one.
“Also importantly, measles during pregnancies have risen dangerously because expectant mothers no longer have lifetime immunity. Today’s vaccinated expectant mothers are at risk because the measles vaccine wanes with time and because it often fails to protect against measles.
“…The danger extends to babies, whose bodies are too immature to receive measles vaccination before age one, making them entirely dependent on antibodies inherited from their mothers. In their first year out of the womb, infants suffer the highest rate of measles infections and the most lasting harm. Yet vaccinated mothers have little antibody to pass on — only about one-quarter as much as mothers protected by natural measles — leaving infants vulnerable three months after birth, according to a study last year in the Journal of Infectious Diseases. [Emphasis mine.]
“Factors such as these increased the death rate for adults and the very young, helping to reverse the decline in deaths seen in previous decades, according to a 2004 study in the Journal of Infectious Disease, authored by researchers at the Centers for Disease Control and Johns Hopkins Bloomberg School of Public Health.”
5. Whenever possible, present the debate as if there are no legitimate reasons to choose not to vaccinate – only “personal beliefs” and “irrational fears.”
The reality is that there are legitimate and documented concerns about vaccine safety. Nobody denies this – all that is in dispute is the magnitude of the harm caused by vaccines. Vaccine manufacturers and their institutional supporters of course insist that any harm from vaccines is minuscule and easily outweighed by the benefits. However this claim is suspect for a number of reasons, not least of which is the stunning degree of conflict of interest and outright fraud within the world of medical research. Leaving aside these issues though, there remain good reasons to distrust the manufacturers’ claims.
Numerous studies fly in the face of the manufacturers’ claims, showing connections between vaccines and autoimmune disease, asthma, allergies, cancer, encephalopathy, and yes, autism. And even assuming integrity in the clinical trial process, these are not sufficient to demonstrate vaccine safety, as they typically only look at reactions that occur within a few weeks of vaccination, and only compare the adverse events experienced with one vaccine against those experienced with another vaccine – not against an unvaccinated sample. Even the Cochrane Review of the literature on the MMR vaccine, for example, came to the conclusion in 2012 that “(t)he design and reporting of safety outcomes in MMR vaccine studies, both pre- and post-marketing, are largely inadequate.”
Studies that purport to demonstrate the safety of vaccines are similarly flawed and limited in their scope. Indeed, of the list of 42 studies put forward by the American Academy of Pediatrics, with an invitation to parents to “examine the evidence”, none compare vaccinated against unvaccinated populations, and most look only at either the MMR vaccine or at Thimerosal.
Meanwhile, because of a law that removes any liability from the makers of vaccines for any harm caused by their products, the Vaccine Injury Compensation Program (VICP) has paid out nearly $3 billion in damages to the families of those who claim they have been injured by vaccines since its inception in 1988. This is despite the elimination by the DHHS of most of the original adverse events from the “Table of Compensable Events”, and what NVIC President Barbara Loe Fisher calls “…a highly adversarial, lengthy, expensive, traumatic and unfair imitation of a court trial for vaccine victims and their attorneys.”
And every year, around 30,000 reports are made to the Vaccine Adverse Events Reporting System (VAERS) which records adverse reactions immediately following vaccination, as reported by doctors, other medical professionals, pharmaceutical companies, patients and parents. Thirteen percent of these are classified as “serious” (including death).
Of course these numbers don’t mean very much without a comparison to the background rate of such adverse events in the general population, not immediately following vaccination. Some studies have shown no increased adverse events after vaccination as compared to the general population. Other studies (including some that use post-vaccination data for other vaccines for comparison, rather than population-wide background rates) show higher rates of adverse events immediately post-vaccine.
Vaccine proponents argue that the VAERS numbers are not an accurate reflection of vaccine damage, because each case reported has not been conclusively proven to be caused by a vaccine. It is a legitimate point – and is largely due to the fact that in most cases there is no way to confirm vaccination as the cause of the event.
The much bigger problem though is the degree to which the VAERS numbers suffer from significant underreporting. Says president of the National Vaccine Information Center and advocate for parental choice regarding vaccines Barbara Loe Fisher:
“There have been estimates that perhaps less than 5 or 10 percent of doctors report hospitalizations, injuries, deaths, or other serious health problems following vaccination. The 1986 Vaccine Injury Act contained no legal sanctions for not reporting [via VAERS]; doctors can refuse to report and suffer no consequences.”Indeed, one study found that while 68% of cases of vaccine-associated polio were reported, only 4% of MMR-associated thrombocytopenia were reported. An earlier study found that only 1% of adverse events following prescription drug use were reported. And in 1994, a survey found that only 18% of 159 doctors’ offices made reports when children suffered serious health problems following vaccination. In New York, this number was one out of 40.
Some argue that adverse events are also over-reported to VAERS, presumably by distraught parents, but this charge is less credible. All the evidence shows that doctors and other healthcare providers are extremely reluctant to report events to VAERS. Healthcare providers account for 36% of all reports to VAERS, with vaccine manufacturers accounting for another 37%. Vaccine recipients and their parents or guardians account for only 7% of reports.
So what is the real risk of overall vaccine injury? The only honest answer is that nobody knows. The number of genuine vaccine injuries is likely much higher than what is reported in VAERS, but how much higher nobody can reliably say. The science on vaccine safety is conflicted, it is insufficient and it is badly corrupted by special interests. It is anything but “settled.”
But there’s more.
There is evidence that vaccines may cause harm well beyond what would show up in an adverse events report – harm that may manifest over many years, rather than in the days and weeks immediately following vaccination. Vaccines have been connected to increased rates of cancer, severe allergies and autoimmune disease:
As Dr. Donald Miller explains:
“Measles helps a child’s immune system grow strong and mature.(The study can be found here.)
“Once past the immunologic barriers of skin and mucosa, our (2-trillion-cell) immune system has two components: An innate system, which all animals have; and an evolutionarily more recent adaptive system that vertebrates have. The childhood diseases—measles, mumps, rubella, and chickenpox—play a constructive role in the maturation of the adaptive immune system. Two kinds of helper T-cells (Th) manage this system:cellular T-cells (Th1); and humoral T-cells (Th2), which make antibodies. The Th1 cellular T-cells are especially important because they attack and kill cells in the body that run amok and become cancerous. And they also kill cells that become infected with viruses.
“Measles (and other viral childhood diseases) stimulate both the Th1 and Th2 components. The MMR vaccine stimulates predominately the Th2 side. Overstimulation of this part of the adaptive immune system provokes allergies, asthma, and auto-immune diseases. Since the Th1 side thwarts cancer, if it does not get fully developed in childhood a person can wind up being more prone to cancer later in life. Women who had mumps during childhood, for example, have been found to be less likely to develop ovarian cancer compared with women who did not have mumps.”
According to the CDC, food allergies in children increased by about 50% between 1997 and 2011. Asthma rates have also been on the rise, with an increase of 28% between 2001 and 2011. And childhood cancer rates have been increasing since the 1970s. The National Institutes of Health reported in 1996 that the incidence of childhood cancer had increased by 10% between 1973 and 1991, and a 1999 report in the International Journal of Health Services said that:
“From the early 1980s to the early 1990s, the incidence of cancer in American children under 10 years of age rose 37 percent, or 3 percent annually. There is an inverse correlation between increases in cancer rates and age at diagnosis; the largest rise (54 percent) occurred in children diagnosed before their first birthday. “There are no definitive explanations for these dramatic increases in potentially life-threatening conditions among children, and in all likelihood there is no single cause responsible for any one of them. However parents have good reason to be concerned about harmful environmental factors, including vaccines. Indeed, several studies show increased rates of immunological problems associated with vaccination.
A study in New Zealand found a higher rate of asthma among those who had been vaccinated (Kemp et al, 1997); Data from the National Health and Nutrition Examination Study in the US showed that children vaccinated with DTP or Tetanus vaccines were twice as likely to develop asthma as unvaccinated children (Hurwitz and Morgenstern, 2000), and another study showed that the MMR vaccine can cause human white blood cells to develop IgE antibodies – one of the main characteristics of asthma (Imani and Kehoe, 2001). A 2008 study found that delaying DPT vaccination was associated with reduced risk of childhood asthma.
Other studies have found a link between vaccines and allergies and autoimmune disease. A 1996 study in Africa found higher rates of allergies among those who had been vaccinated against measles than among those who had survived the disease. The study concluded that “(m)easles infection may prevent the development of atopy in African children.”
A 2001 study confirmed “A causal association between measles-mumps-rubella (MMR) vaccine and idiopathic thrombocytopenic purpura (ITP)…”; A study in 2014 found a strong correlation between hepatitis B vaccination and higher rates of multiple sclerosis; a 1999 study in Japan found that “…gelatin-containing DTaP vaccine may have a causal relationship to the development of this gelatin allergy”; and in 2009, a Japanese study that gave mice repeated immunizations with antigen found that “(s)ystemic autoimmunity appears to be the inevitable consequence of over-stimulating the host’s immune ‘system’ by repeated immunization…”
In the journal Autoimmunity, Vared Molina and Yehudi Shoenfeld write “Vaccines, in several reports were found to be temporally followed by a new onset of autoimmune disease. The same mechanisms that act in infectious invasion of the host, apply equally to the host response to vaccination. It has been accepted for diphtheria and tetanus toxoid, polio and measles vaccines and GBS. Also this theory has been accepted for MMR vaccination and development of autoimmune thrombocytopenia, MS has been associated with HBV vaccination.”
Those who would force vaccinations on the rest of us are fond of repeating bromides like “your right to be sick ends where public health begins.” But who gets to decide what constitutes “public health”? Who decided that the eradication of every childhood illness is in the best interests of “public health”? Why are not increased rates of childhood cancer and life-threatening allergies relevant to “public health”? Why can I not demand that everyone else stop vaccinating their children because doing so directly threatens the ability of mine to contract childhood diseases which might help strengthen their immune systems?
6. If you must acknowledge that critics of vaccines have actual reasons for their concerns, restrict the discussion to the fear that vaccines may cause autism, and be sure to stress that the only basis for this concern is the retracted 1998 study by Andrew Wakefield.
You can also mention some of the studies that “prove” there is no causal link between vaccines and autism. Just be sure not to mention any of the ones that do show a connection, like this one, this one or this one. Be especially careful not to mention this one, this one, or any of these, these or these.
At all costs, never ever mention any of the concerns listed in “4.” above.
For bonus points, see if you can create the impression that the only potential problem with vaccines is thimerosal, and then declare that thimerosal has been removed from all vaccines. (It hasn’t.)
7. When in doubt, pepper your stories with some of the following affirmations. Remember: The more you say them, the truer they become: “Vaccines save lives”; “parents who don’t vaccinate are selfish” (“ignorant”, “anti-science” and “hippies” all work well too.); and above all: “the science is settled.”
You may have to repeat this last one many many times before your readers come to understand and accept it.
8. Don’t even address vaccines directly. Simply include some mention of vaccine skepticism as an example of the kind of irrational thinking some people (especially, strangely, well-educated ones) still engage in despite “everyone knowing” how foolish it is.
This is perhaps the most powerful tool you can use to sway your audience. Nobody wants to be seen as foolish, and most people don’t have the time or inclination to look closely at the evidence for and against vaccine safety. If people keep hearing that “everyone knows” vaccines are safe and effective, most of them will tend to go along with that position even if they don’t know much about the topic – if only to avoid being seen as crackpots. Fear of public humiliation can be a beautiful thing in the right hands.
9. If the icky topic of conflict of interest or corruption of the research by vested interests comes up, just laugh it off. Remember: Writing in a derisive tone about other people’s claims or concerns is exactly the same as refuting them.
Amy Wallace, who wrote this Wired piece handled this especially well. And not only did she fail to interview a single critic of vaccines for the article, she cunningly created the impression that she had included their views by visiting an Autism One conference and mentioning and briefly quoting – but never actually speaking with – NVIC president Barbara Loe Fisher. Well done Amy Wallace!
Be sure to quote Dr. Paul Offit and to cite him as a “vaccine expert”. Don’t bother disclosing that he has made millions of dollars from the Rotavirus vaccine he developed. The whole notion of disclosing conflicts of interest within a story is so passé. Also anti-science.
Vaccine advocates like to point to studies that show no increased risk of harm from vaccines. They assert that these studies invalidate the findings of other studies that do show a link between vaccines and asthma, allergies, autism and other conditions. In a world in which scientific institutions could be trusted to conduct honest, objective research and produce credible results, this might provide some comfort. In the real world though, there is little reason to give credence to much of the research that gets produced on vaccines – and much less so to results that in any way favor the manufacturers of those vaccines.
Lest anyone suspect that this kind of cynicism about the scientific establishment is confined to anti-vaccination activists, here is what Marcia Angell, former editor in chief of the New England Journal of Medicine, wrote in 2009:
“…(C)onflicts of interest and biases exist in virtually every field of medicine, particularly those that rely heavily on drugs or devices. It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of TheNew England Journal of Medicine.” [Emphasis mine.]Angell adds:
“No one knows the total amount provided by drug companies to physicians, but I estimate from the annual reports of the top nine US drug companies that it comes to tens of billions of dollars a year. By such means, the pharmaceutical industry has gained enormous control over how doctors evaluate and use its own products. Its extensive ties to physicians, particularly senior faculty at prestigious medical schools, affect the results of research, the way medicine is practiced, and even the definition of what constitutes a disease.”Likewise, in his 2013 book “Bad Pharma”, physician (and vaccine advocate) Ben Goldacre writes:
“Overall, the pharmaceutical industry spends around half a billion dollars a year on advertising in academic journals. The biggest – NEJM, JAMA – take $10 or $20 million each, and there is a few million each for the next rank down.”Goldacre adds that “(a)dvertising is not the only source of drug company revenue for academic journals”, and cites “supplements” – special editions sponsored by drug companies – and reprints of individual academic papers that can bring in up to a million dollars each. And he cites a 2009 study demonstrating that industry-funded studies are more likely to be accepted by journals.
The real-world impact of this control has been well documented, from the FDA concealing fraud in medical trials, to built-in biases in studies, to pharmaceutical companies misleading practitioners as to the safety and efficacy of their products, to allegations of fraudulent misconduct brought by scientists turned whistleblowers.
Recently, two former Merck scientists charged that the pharmaceutical giant “…fraudulently misled the government and omitted, concealed, and adulterated material information regarding the efficacy of its mumps vaccine…” And in August of last year, senior CDC scientist William Thompson came forward with the statement that he and other researchers had omitted statistically significant data from a 2004 article published in the journal Pediatrics. (It is worth noting that Dr. Thompson’s earlier studies at the CDC were hailed as “definitive” in refuting the Thimerosal-autism link by none other than Dr. Paul Offit.)
According to Thompson’s statement “(t)he omitted data suggested that African American males who received the MMR vaccine before age 36 months were at increased risk for autism. Decisions were made regarding which findings to report after the data were collected, and I believe that the final study protocol was not followed.”
In a secretly recorded conversation, Dr. Thompson told with Dr. Brian Hooker, “I have a boss who is asking me to lie. The higher ups wanted to do certain things and I went along with it.” He told Dr. Hooker that “…the CDC has not been transparent, we’ve missed ten years of research, because the CDC is so paralyzed right now by anything related to autism. They’re not doing what they should be doing. They are afraid to look for things that might be associated…”
Put simply: The scientific establishment has lost any right to be taken at its word on this issue.
10. “Muh Herd Immunity!”
Remind your readers of our long-treasured right to herd immunity: The right to demand – at gunpoint if necessary – that others take every possible precaution against contracting communicable diseases, regardless of the risks to themselves of doing so. This is a right our forefathers fought and died for and we’re not about to give it up now.
Actually, no.
Those who support imposing vaccines by force argue that those who do not vaccinate threaten herd immunity for the entire population. The idea that vaccines can successfully provide herd immunity is already questionable, as – unlike many childhood diseases – they do not confer lifetime immunity. Nor do they offer 100% immunity to those vaccinated. But more importantly this argument presumes that “herd immunity” is something anyone has a right to in the first place.
For centuries, people have been aware that being out in public carries certain risks – among them, the risk that one might contract a disease from another person. Never before have people widely asserted that they have the right to demand that everyone around them take all possible precautions at whatever cost to themselves to make this environment absolutely risk free. If, as the mandatory vaccination proponents contend, we can demand that everyone around us take every conceivable precaution against every communicable disease, what else can we demand of them?
For starters, the recently vaccinated (with live-virus vaccines) should be excluded from all public property. And if not, why not? They pose far more of a risk than does anyone who has simply not been vaccinated. What are some other risky practices Americans should no longer tolerate from each other? Going out in public with a cold? Being a poor driver? Being in possession of any substance that might cause a severe allergic reaction in someone else?
How about superbugs? What are we going to do about all those people who abuse antibiotics, ultimately leading to the creation of superbugs. Antibiotic-resistant bacteria are responsible for nearly 15,000 deaths in the US each year, far outstripping pre-vaccine deaths for measles, mumps and whooping cough combined. Can we not hold the irresponsible people who take antibiotics every time they have a minor infection accountable for this?
Personally, I avoid antibiotics for myself and my family as much as possible. I have never given them to a child with an ear infection (and yes, we’ve had some.) Should my preferences be imposed on everyone else? Doing so would clearly strike a blow against the propagation of superbugs. So why not?
Here’s why not: Because your right to protect “public health” – whatever you think that may be given the interest-driven media hysteria of the moment – ends where my body begins.
Herd immunity is not something anyone has a “right” to. It is a positive externality, and like other such externalities it is not something you have a right to demand that your fellow human beings provide for you. More to the point, you do not have a right to demand that other parents impose risks on their children that they are not comfortable with, in order to protect your child or anyone else’s children.
The Forced Vaccination Threat: a Tragedy of the Commons
Can there ever be a point where spreading a disease becomes “assault”? Of course there can: A person who knows that they are infected with Ebola, for example, stepping into a crowded subway car and proceeding to cough all over the other passengers, could easily be considered guilty of assault. But measles is hardly Ebola (it is not even on the federal government’s list of quarantinable diseases), and – contrary to the media frenzy that insists otherwise – not being vaccinated does not equate to being infected with a disease, far less to knowingly infecting others. Failure to take every precaution against getting a disease is hardly “assault.”
Even in the case of a truly deadly illness like Ebola, there is no justification for forcing a particular method of prevention on those who have not contracted it, or forcing treatment on anyone who has. All that anyone has a right to do is demand that those people not infect others.
It should be obvious by now that none of this would even be an issue if we lived in a society that honored self-ownership and private property. In the event of an outbreak of a truly dangerous disease – or even a disease that posed a serious risk to only a small segment of the population – each property owner could make their own decision about whether to exclude those who were infected or indeed, even those who chose not to be vaccinated against the disease, presuming there was a vaccine for it.
As economist Robert Murphy writes:
“Private businesses aren’t stupid; they don’t need the government to order them to keep lepers away. And if a particular church, say, wants to open its doors to such a person, that’s perfectly within their rights. (As a matter of courtesy, we would hope this policy would be announced to others who might not want to visit the same building.) Indeed, the final repository for such people would be buildings where the owners thought they could safely contain the disease. And the common name people would use for these buildings is “hospital.” In a free society, to be “quarantined” would simply mean that most owners (of roads, sidewalks, malls, hotels, factories, etc.) would refuse access, and so a contagious person would have few choices outside of treatment facilities.”Rather than having a one-size-fits-all solution imposed upon everyone by some authority, everyone would make choices based on their own perception of the risks. Businesses that responded to the risk sensitivities of their customers would do well and those that did not would suffer. And because not all people have the same perception of or sensitivity to the same risks, there would be a wide variety of choices: Schools that allow unvaccinated children and schools that do not; restaurants that cater to those with severe allergies and those that do not; parks, libraries, cinemas and other establishments that specialize in serving immunocompromised and other medically fragile individuals, and those that do not.
In the absence of a “commons” – property that is used by everyone but owned by no-one (or, more realistically, owned by the state) there would be no calls for anyone to have vaccines forced upon them at gunpoint. Those who believe vaccinations are absolutely necessary would frequent businesses and venues that enforced strict vaccination policies, and those who did not would frequent places that had more relaxed policies.
My own guess is that for the most part, the issue would simply go away. People would come to realize that the real risk to themselves and their families posed by those who do not vaccinate is in fact minuscule – particularly in comparison to other risks we all expose ourselves to daily. In the absence of a “commons” managed by people who do not have to earn the costs of their operation, most business owners would find that they stood to lose more by excluding “non-vaxxers” than they did to gain by allowing them in.
It is only in a world where property rights are not clearly defined, where there are great swathes of “commons” (either “public” property or nominally private property over which owners do not have genuine decision-making powers) that there can be a conflict between “public” health and individual rights. Eliminate the commons and you eliminate that conflict – replacing it with a myriad of voluntary solutions to meet the differing wants and needs of diverse individuals.
Whatever Your Views on Vaccines, the Prospect of Forced Vaccination Ought to Make You Very Very Afraid
Do those who believe in mandated vaccination really want to establish the precedent of granting a government body the power to compel people to be injected with substances against their will? You may support the forced vaccination of other people’s children because you think vaccines are undeniably beneficial and problem-free. But you may not be so thrilled about the next substance the state decides everyone should have forced into their veins.
Do you really want to establish the precedent of being able to demand from your neighbors that they pose no risk to you at all? The corollary of course being that they may then demand the same of you? If as a society we decide that we have the right to demand a 100% risk-free environment in which to live then the potential intrusions into our lives are infinite.
Even if the manufacturers’ claims are correct and the risk of serious injury from vaccines is infinitesimal, for most people it is impossible to know ahead of time whether or not they will be injured by a vaccine. Nobody has the right to force another person to choose that risk – however small it may be – over the risks of the diseases the vaccines are intended to prevent.
The state already controls vast swathes of what we can do with our lives: What professions we may enter, how and where we may conduct business, what substances we cannot ingest, how much of the money we earn we are allowed to keep, how we may travel and what indignities we must tolerate in order to do so, when and where we may protest, and the list goes on and on. If you do not believe that individuals have the right to control what goes into their own bodies then I have to wonder what rights – if any – you do believe people still have.
It seems to me that, save choosing our mates for us, the last remnant of our self ownership lies in our right not to be directly assaulted, not to have unwanted drugs or other substances forced into our bodies. If you believe that the state has the right to do this, then there is essentially nothing left that it does not have a right to do.
The pro-vaccine lobby has done a phenomenal job of inciting fear among the American public in a way that happens to serve its interests: Fear of little children who may not have been vaccinated; fear of other parents who may make choices different from yours; fear of a disease that in the developed world is far less deadly than lightning strikes. But they’ve left out one of the most frightening specters of all, one that has a truly horrifying historical record of death and destruction: An all-powerful state that can literally do whatever it wishes to those living under it. If that prospect frightens you less than the remote possibility that you might contract measles from my five year old, then quite frankly you scare the hell out of me.